Printable Cms 1500 Form 02 12

Cms 1500 Claim Forms Hcfa Version 02 12 1 Part Laser Pkg Of 500

New Cms 1500 02 12 Claim Form 25 Forms

New Cms 1500 Claim Forms Hcfa Version 02 12 100 Per Ream
Its important to adhere to certain guidelines when completing the form to ensure your claims are processed smoothly and quickly.
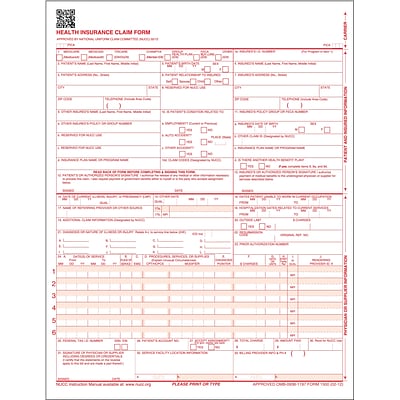
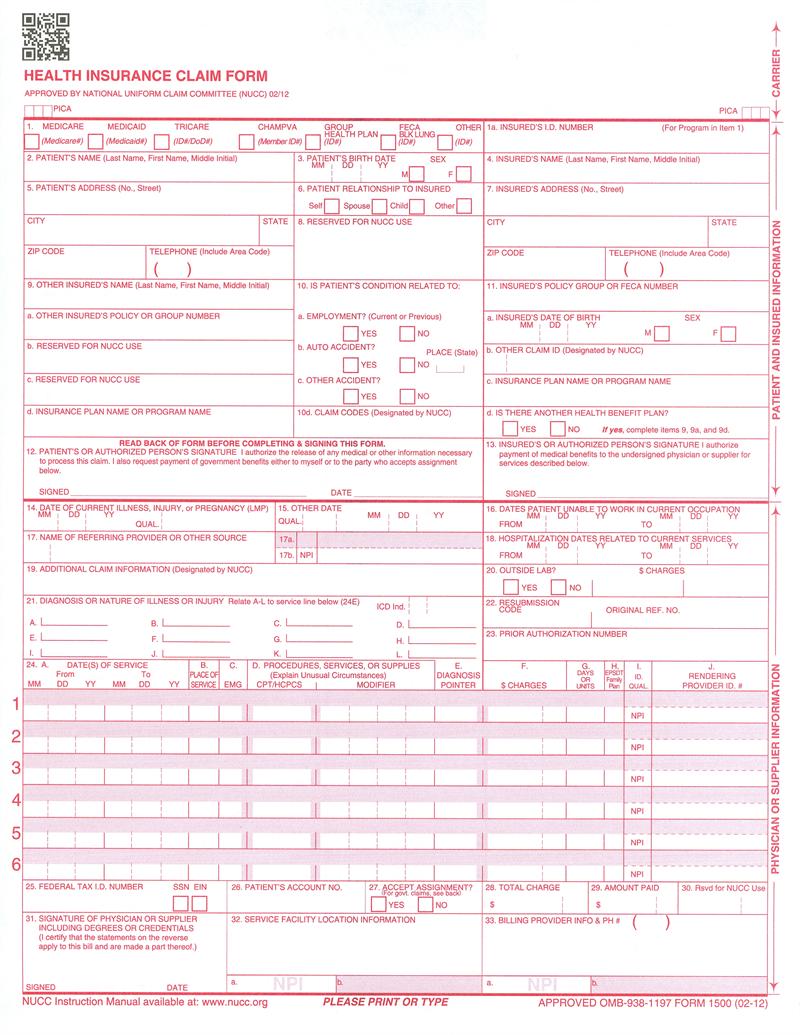
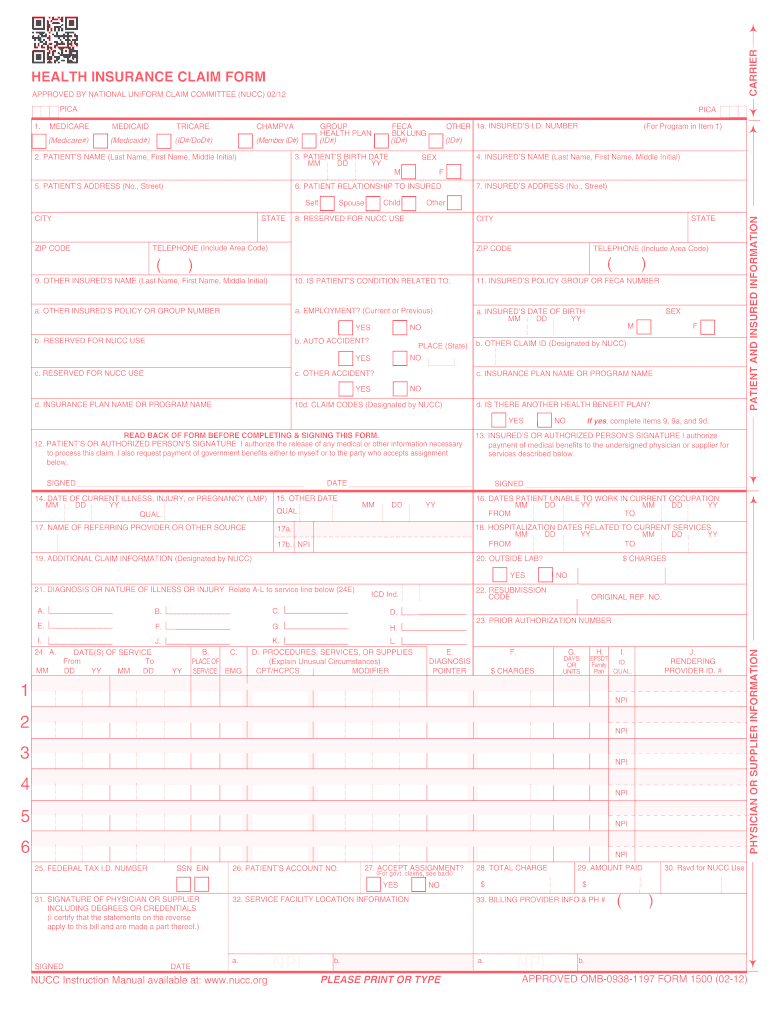
Printable cms 1500 form 02 12. Please print or type approved omb 0938 1197 form 1500 02 12. Centers for medicare medicaid services. The cms 1500 form is the standard paper claim form used by a non institutional provider or supplier to bill medicare carriers and medicare administrative contractors macs when a provider qualifies for a waiver from the administrative simplification compliance act asca requirement for electronic submission of claims. Print the back side as well to ensure the claim will be accepted.
Cms 1500 pdf home a federal government website managed and paid for by the us. Resubmitting a denied claim is not considered an adjustment or void. Insureds date of birth b. Type print and save your claim using a mac or pc.
7500 security boulevard baltimore md 21244. Insureds address no street city state zip code telephone include area code 11. The cms 1500 is a standard form used to transmit healthcare claims and is used by pinnacol assurance for processing claims. The cms hcfa 1500 form is the standard paper claim form used by a non institutional provider or supplier to bill medicare carriers and medicare administrative contractors macs when a provider qualifies for a waiver from the administrative simplification compliance act asca requirement for electronic submission of claims.
Patient s name last name first name middle initial f 6. Insureds policy group or feca number a. Please print or type approved omb 0938 1197 form 1500 02 12 carrier health insurance claim form approved by national uniform claim committee nucc 0212 pica medicaid tricare id dod group health plan id champva medicaid member id feca blk lung 3. Insureds name last name first name middle initial 7.
The cms 1500 pdf hcfa 1500 pdf is used by all health care providers to bill for services. Updated 12242018 cms 1500 02 12 claim form instructions pv07272017 2 adjustmentvoid reason codes for field 22 to adjust or void a previously paid claim use an adjustment or void reason code to complete the code area of field 22 resubmission code. Free hcfacms 1500 form template for medical claims in fillable format. Approved omb 0938 1197 form 1500 02 12 1a.
Download the fillable hcfa 1500 claim form that is both a fillable andor printable medical claim form that will provide insurance illness and injury information for medical services claimsif the user would like to complete the form online simply download click inside the box to begin and begin typing your information. Patient s birth date dd yy mm 2.
Complyright Cms 1500 Health Insurance Claim Form 02 12 Laser Cut Sheet 250 Box

Complyright Cms 1500 Health Insurance Claim Form 02 12 Laser Cut Sheet 8 1 2 X 11 White Case Of 250 Item 486182

New 2012 Cms 1500 Insurance Claim Form

Cms 1500 Form New 02 12 Version Laser 8 5 X 11 2500 Bx

Just Cms 1500 Forms New Blank Cms 1500 Hcfa Form Version
Cms 1500 Health Insurance Paper Claim Forms 02 12 Free Priority Shipping

Cms 1500 Hcfa Claim Forms 02 12 Laser 5000 Count
Cms 1500 Insurance Claim Form
2012 2020 Form Cms 1500 Fill Online Printable Fillable
Details About Cms Hcfa 1500 Health Insurance Claim Forms 25 Sheets 02 12 Version

Cms1500 Claim Forms Version 02 12

Just Cms 1500 Forms New Imprinted Cms 1500 Hcfa Form

New Cms 1500 Claim Forms Hcfa Version 02 12 500 Sheets

New Cms 1500 Form One Part Cms 1500 Continuous Claim Form

2500 Laser Cms 1500 02 12 Insurance Hcfa Claim Forms

1b Cms 1500 Insurance Claim Form Ver 02 12

Cms 1500 Claim Forms Hcfa Version 02 12 2 500 Sheets Approved Omb 0938 1197

New Cms 1500 Form 02 12 Health Forms Systems Inc
