Medicare Claim Form Printable

Medicare Claim Form Fill Online Printable Fillable

Medicare Claim Form Medical Claim Can Be Submitted Through
Free Claim Forms

Get this form in spanish.
Medicare claim form printable. Please read all instructions prior to submitting a claim to medicare. This form can also be used to claim gap benefits from your private health fund for in hospital and ancillary services. There are also forms for filing an appeal or letting medicare share your personal health information. Fill out the patient request for medical payment form cms 1490syoull find the address for form submission in the instructions.
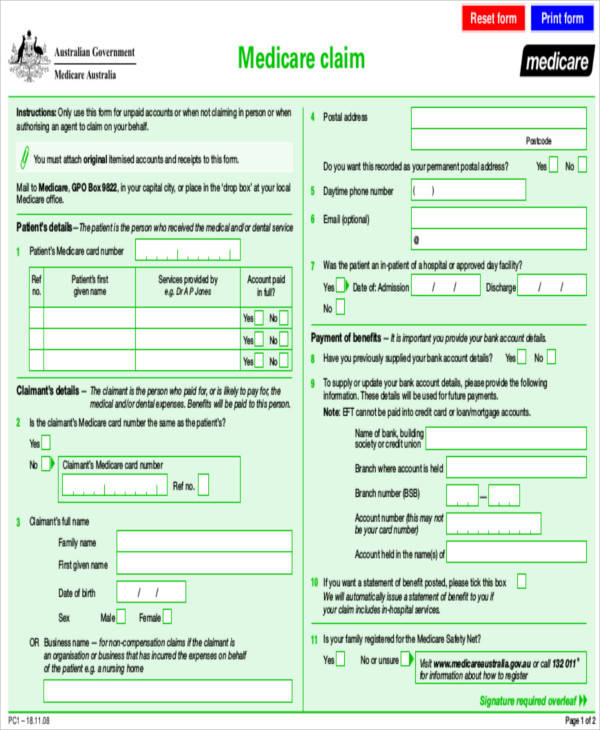
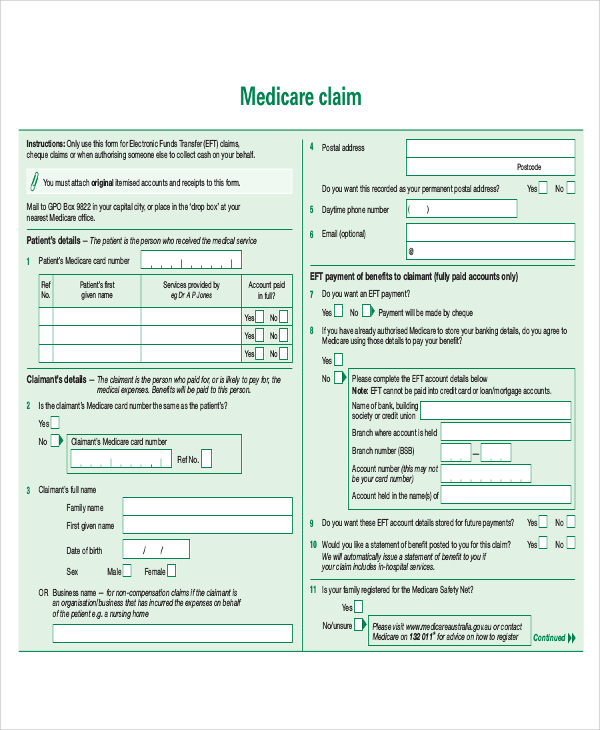
Be sure to attach the superbill or invoice and any receipts of your payments. Filling out your claim form. Fill out this form if you were billed directly by a provider and would like to request reimbursement for medical care includes dental vision hearing and vaccines. We pay medicare benefits directly into your nominated bank account.
Effective april 1 2019 only the revised 01 18 version will be accepted for the form cms 1490s. Medicare administrative contractor address table for the correct address to mail your claim form. If you still do not know the address of your medicare contractor call 1 800 medicare 1 800 633 4227. Dont include this instruction page with your faxed or mailed claim form.
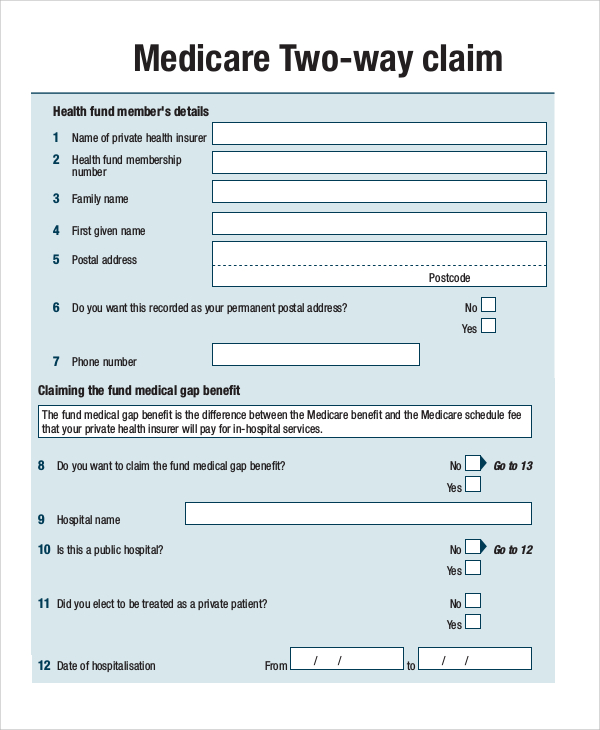
Please print or write legibly when completing the account holder first and last name. Please include your bank details on the form if we dont have them or if they need updating. Medicare two way claim form ms001 use this form together with a medicare claim form to submit your in hospital and ancillary claims with medicare and your private health fund. Once you have completed the form mail it to the address listed on the back of your health plan id card.
The provided link below includes the form and all the applicable instructions. Medicare forms get medicare forms for different situations like filing a claim or appointing a representative. Medicare claim form ms014 use this form to claim medicare benefits by mail or in person at a service centre. Medicare reimbursement account mra claim form instructions how to submit claims by fax or mail.
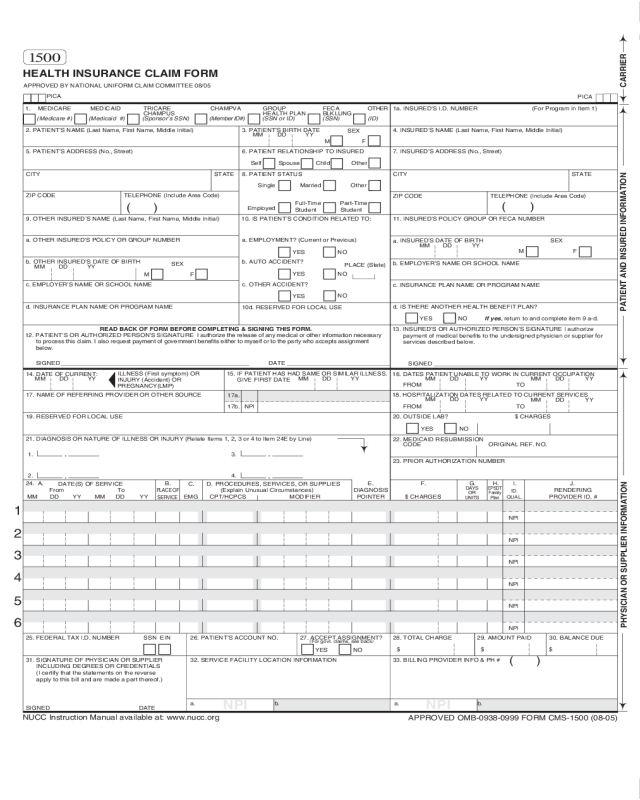
1 the form cms 1490s is fillable can be completed online printed then mailed. This pdf is fillable. Print a prescription drug claim form spanish print and complete this form for medical dental vision hearing or vaccine reimbursement.
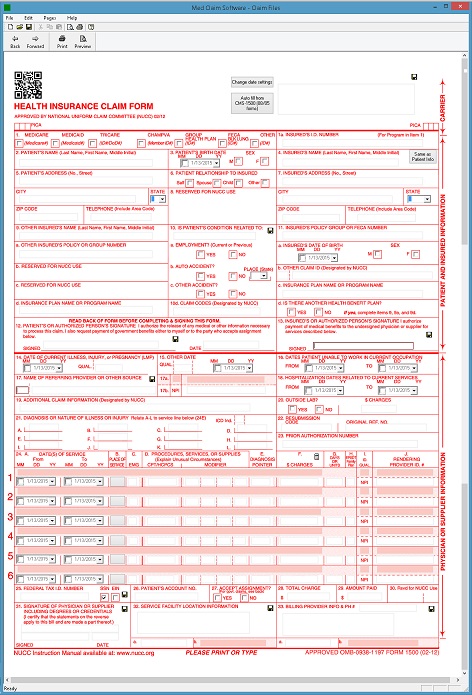
Cms 1500 Health Claim Form Software 79
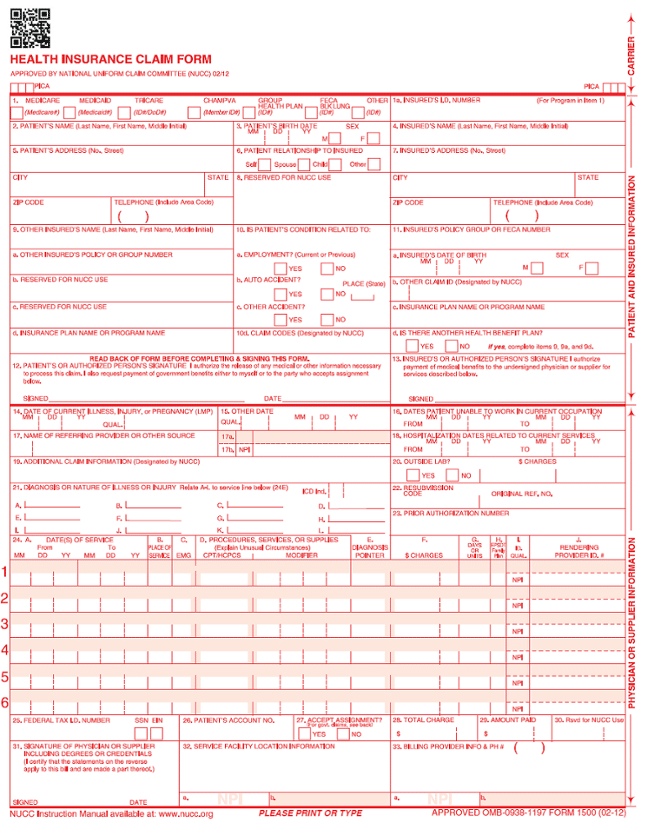
Cms 1500 Template
41 Million Medical Claims Rejected By Medicare In 1 Day
Sample Medicare Form 8 Examples In Word Pdf
Sample Medicare Claim Form Templates Printable Medical
Sample Medicare Claim Form 9 Examples In Word Pdf
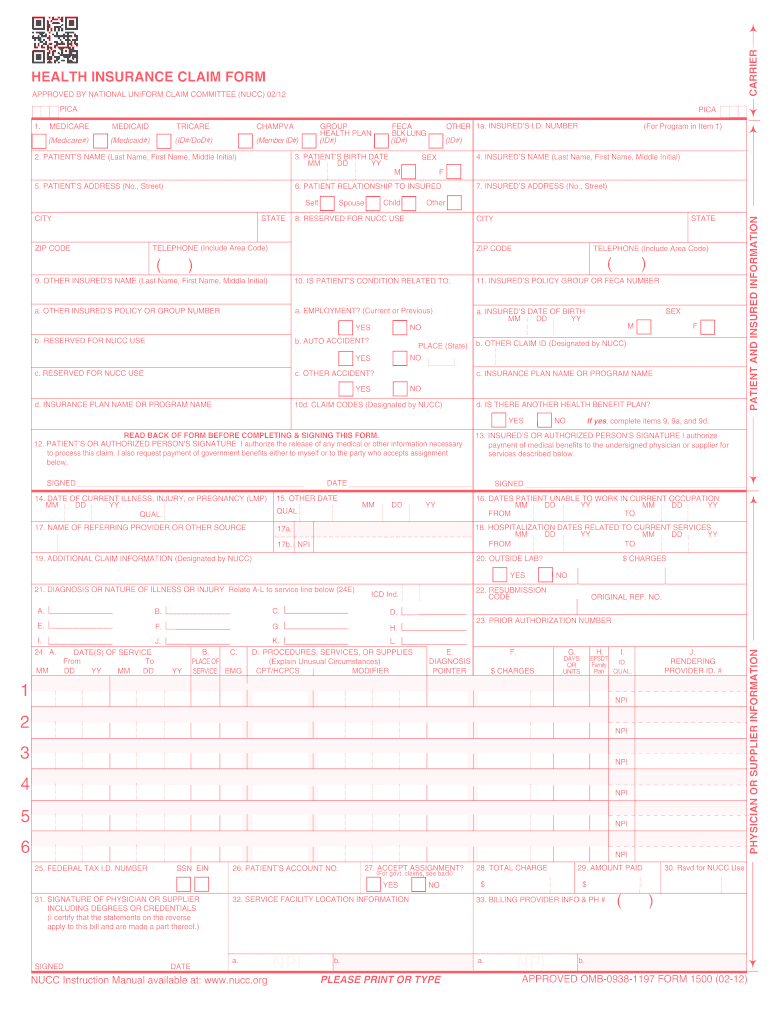
2012 2020 Form Cms 1500 Fill Online Printable Fillable
Sample Medicare Claim Form Templates Printable Medical
Insurance Claim Sample Form Edit Fill Sign Online Handypdf

Sample Medicare Claim Form 9 Examples In Word Pdf

1500 Claim Form Free New Cms 1500 Blank Paper Claim Form
/CMS-1500-claim-form-57a2d3a85f9b589aa99caf8b.jpg)
Cms 1500 Claim Form Versions And Tips

Fillable Medicare Reimbursement Form Fill Online

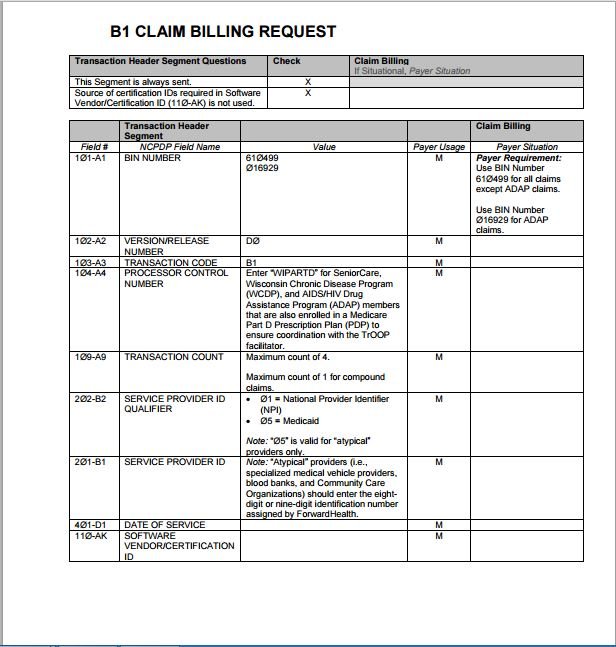
Tmppm 2010 6 5 3 Cms 1500 Blank Claim Form
Medical Billing Process Cms 1500 Claim Form Billing Instruction

Cms 1500 Claim Form Versions And Tips
Sample Medicare Form 8 Examples In Word Pdf

Medicare Claim Form Cms 1490s Form Resume Examples
